Millions taught the signs of breathing emergencies. Told deny God’s ‘Breath of Life’ (rescue breaths) give chest compressions a beating heart. Murder both counts
State sponsored psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Done on purpose Be safe. Be kind. First, do no harm @GaryCPR
Barbara Jaffe MD Associate Medical Officer of Health Ontario and Mayor John Tory quoted “Ventilations (rescue breaths) most important” “This (wrong protocols) is what causes people to lose their lives quite literally” Both know they could be next needlessly in the morgue suffer any of the 100s of causes breathing emergency https://youtu.be/2Pb0HAPqWII
2010 AHA Guidelines part 12:7 ‘Toxic Ingestions’ Toxidromes Quote “Practically every sign and symptom observed in poisoning can be produced by natural disease, and many clinical presentations associated with natural disease can be mimicked by some poison.” [means signs of OD can mimic any breathing emergency caused by illness or injury rescue breathing only ASAP diagnose then treat the underlying cause]
Opioid Toxicity “Naloxone has no role in the management of cardiac arrest” “ventilation should be assisted by a bag mask [rescue breaths same] followed by administration of naloxone and placement of an advanced airway [rescue breathing same] if there is no response to naloxone.” [Naloxone fails to work many cases kept alive with breaths only as in any breathing emergency breaths only ASAP] https://www.ahajournals.org/doi/full/10.1161/circulationaha.110.971069
VI. First Aid Awareness and Training Providers of First Aid Training in Ontario, including St. John Ambulance, Canadian Red Cross, and Heart and Stroke Foundation of Canada, should:
i Ensure their standard first aid training programs and their instructors: emphasize the primary importance of airway patency and positional safety for all ill and injured patients
Original story SHERIFF FIGUEROA’S RESPONSE TO THE RECENT INCIDENT IN THE TOWN OF ULSTER NY https://www.facebook.com/UlsterSheriff/videos/439367593906712First line Police quote “I found it prudent to release” Gary Thompson “I found it essential release info Police etc. are teaching murder”
My original comment She is a nurse knows the cops are teaching murder Blue lives murder their own everyone One minute video comment box has the medical infohttps://youtu.be/OSQcZnAM7Yk
Assistant Chief Police knows what a child knows Breathe once every five seconds or die
Blue lives murder their own everyone One minute video Life threatening training in comment box https://youtu.be/OSQcZnAM7Yk
Nashville “Do not give mouth to mouth these victims please” “Give chest compressions only” A BEATING HEART? Last minute of video Kentucky rescue breaths saves any breathing emergency https://youtu.be/8kWogvCwI9s
Michael Dailey MD Medical Directory New York State quote “our law enforcement education does not include a recommendation for ventilation, but asks departments to train their officers on CPR and for it to be preformed, with no statement about hands’ only or breathing techniques.”
Phone call Dec 28, 2020 Cathedral of the Immaculate Conception Albany NY Where is the righteous indignation? https://youtu.be/LQlyPnr5be4
Saint Joseph’s University Institute of Clinical Bioethics liked my comment “This injustice negates all things positive, speak up” https://youtu.be/UEODnKr2GYw
My phone call White House Secret Service agents have First Aid know millions have been taught murder https://youtu.be/eQUrEyi4f34 Comment boxes medical info
State sponsored psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Done on purpose Be safe. Be kind. First, do no harm @GaryCPR
Over a million people overdosed per day for surgery using many different substances including opioids the only thing keeping patient alive is ventilations (rescue breaths same for layperson). Millions trained deny rescue breaths give compressions only or CPR.Increases morbidity and mortality any respiratory emergency caused by illness or injury.
Top 10 Take-Home Messages for Adult Cardiovascular Life Support
6. The opioid epidemic has resulted in an increase in opioid-associated out-of-hospital cardiac arrest, with the mainstay of care remaining the activation of the emergency response systems and performance of high-quality CPR. [Cardiac arrest secondary respiratory arrest prognosis very poor. Patient needs Advanced Cardiac Life Support methods See my references 1-1a Reference 2015 AHA Guidelines 10:3 page 504-6 ]
Special Circumstances of Resuscitation
Opioid Overdose
The ongoing opioid epidemic has resulted in an increase in opioid-associated OHCA, leading to approximately 115 deaths per day in the United States and predominantly impacting patients from 25 to 65 years old.1–3 Initially, isolated opioid toxicity is associated with CNS and respiratory depression that progresses to respiratory arrest followed by cardiac arrest. Most opioid-associated deaths also involve the coingestion of multiple drugs or medical and mental health comorbidities.4–7
In creating these recommendations, the writing group considered the difficulty in accurately differentiating opioid-associated resuscitative emergencies from other causes of cardiac and respiratory arrest. Opioid-associated resuscitative emergencies are defined by the presence of cardiac arrest, respiratory arrest, or severe life-threatening instability (such as severe CNS or respiratory depression, hypotension, or cardiac arrhythmia) that is suspected to be due to opioid toxicity. In these situations, the mainstay of care remains the early recognition of an emergency followed by the activation of the emergency response systems (Figures 13 and 14). Opioid overdoses deteriorate to cardiopulmonary arrest because of loss of airway patency and lack of breathing; therefore, addressing the airway and ventilation in a peri arrest patient is of the highest priority. The next steps in care, including the performance of CPR and the administration of naloxone, are discussed in detail below.
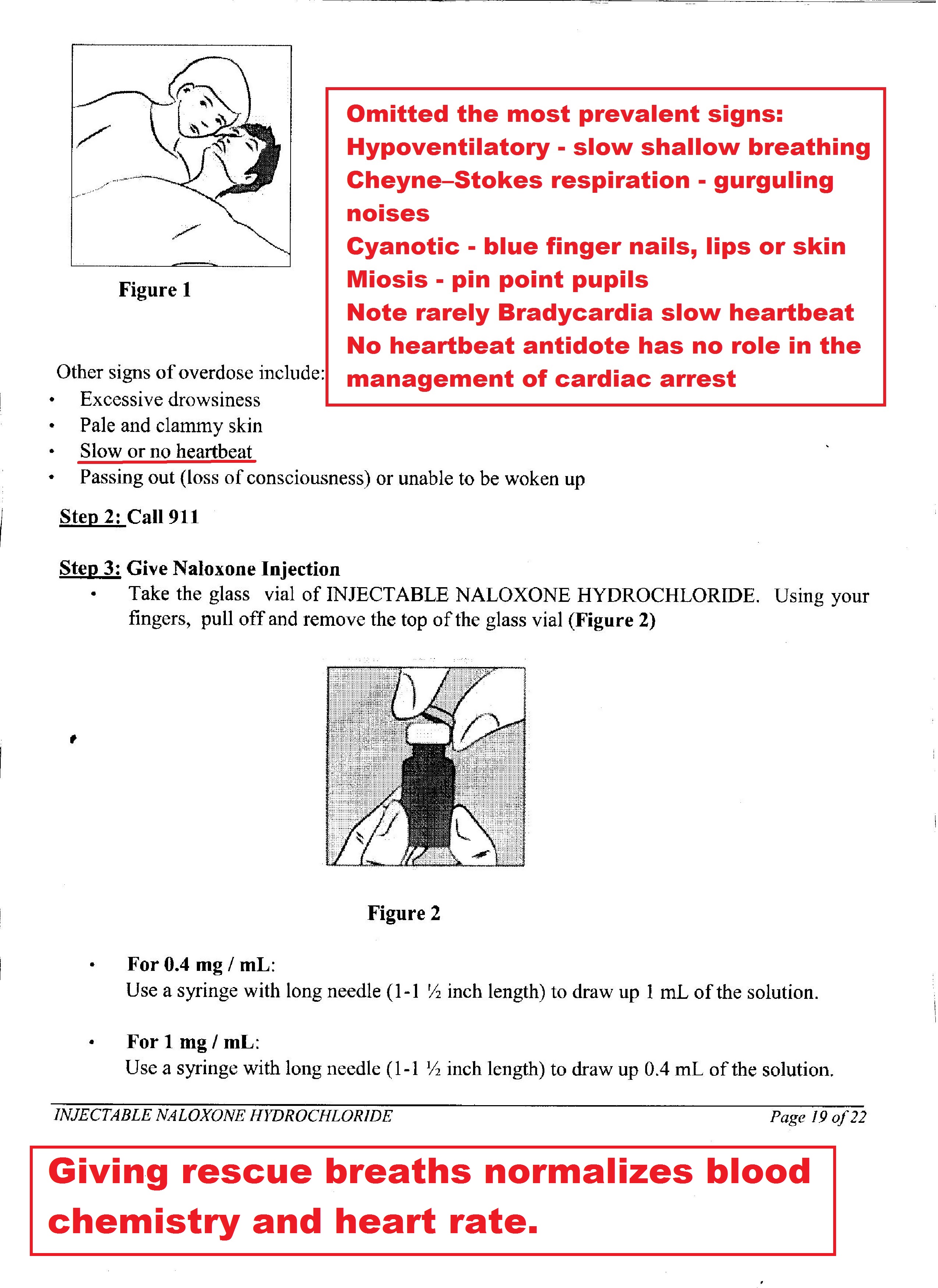
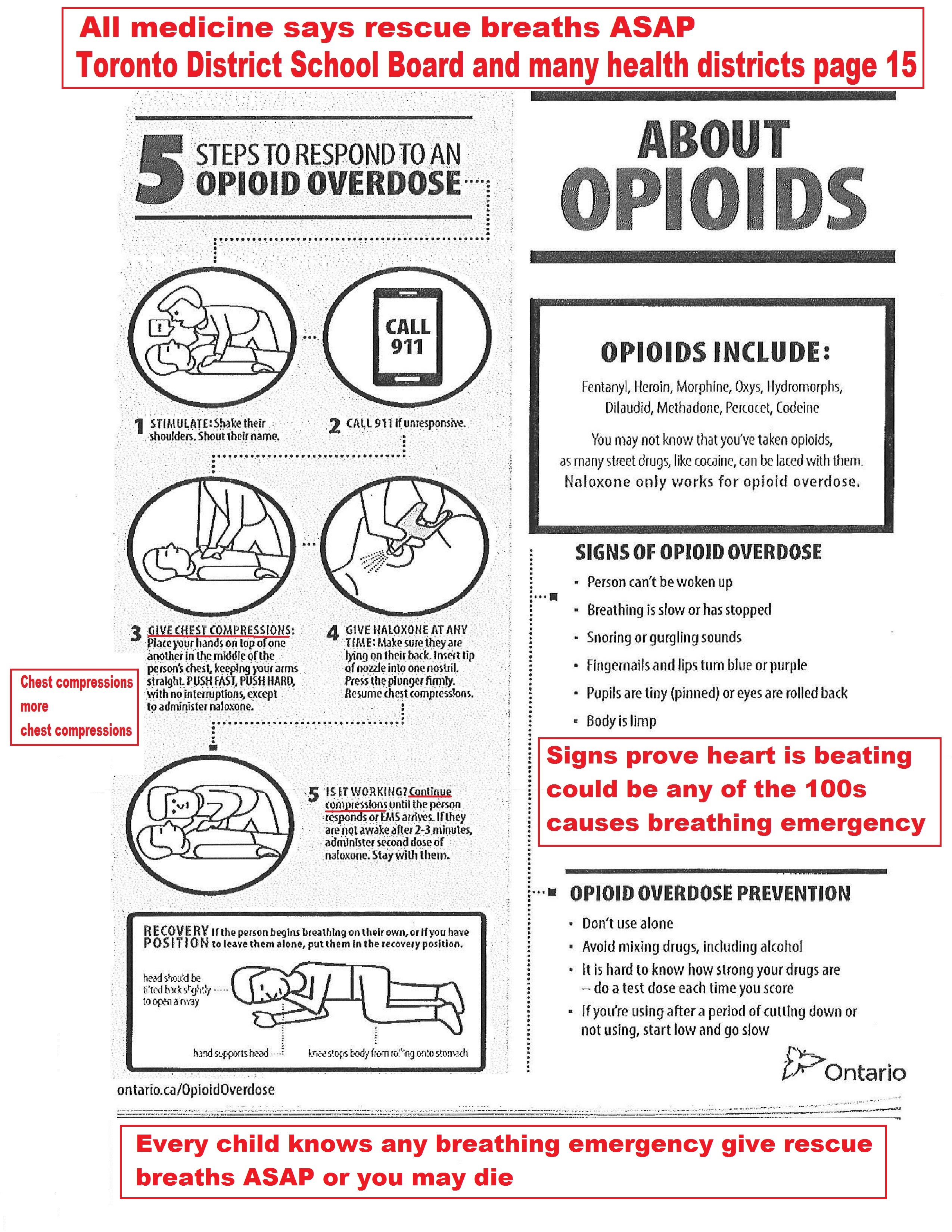
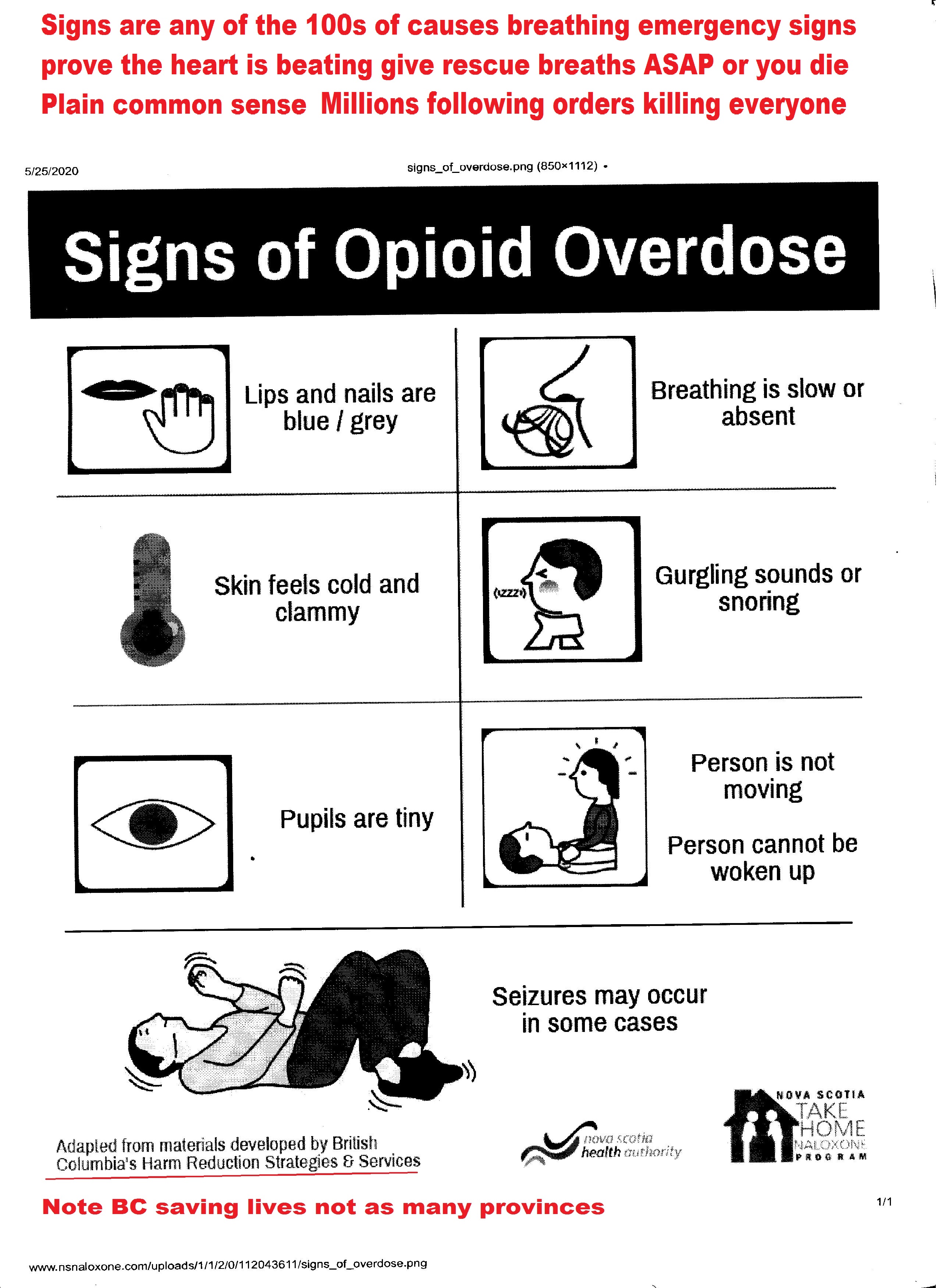
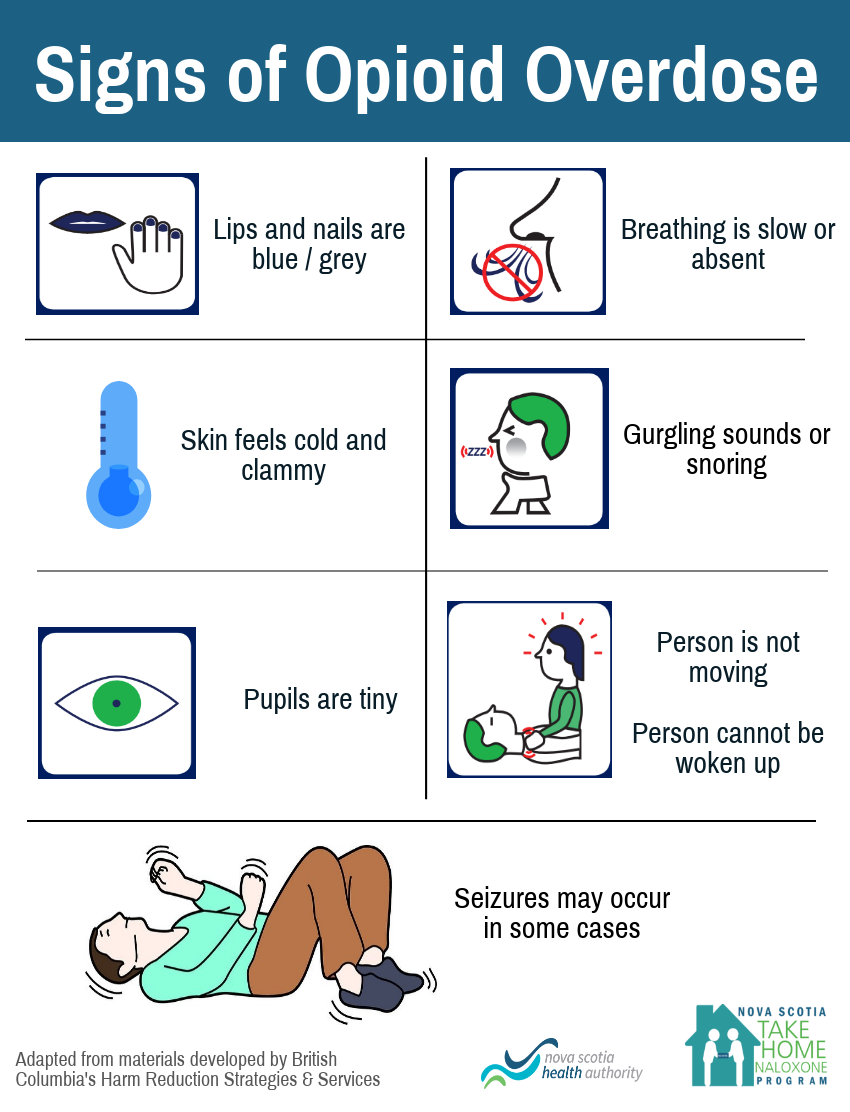
Signs OD taught to millions comatose; hypoventilatory; Cheyne-Stokes respirations; cyanotic; miosis all proves the heart is beating rescue breaths essential, pre naloxone and post administration. Signs of OD can mimic any of the 100s of causes breathing emergency. Naloxone has no role in the management of cardiac arrest Naloxone does not work in many cases italics mine
Figure 13.Opioid-Associated Emergency for Lay Responders Algorithm. AED indicates automated external defibrillator; CPR, cardiopulmonary resuscitation; and EMS, emergency medical services.
Figure 14.Opioid-Associated Emergency for Healthcare Providers Algorithm. AED indicates automated external defibrillator; and BLS, basic life support.
Additional recommendations about opioid overdose response education are provided in “Part 6: Resuscitation Education Science.”Recommendation-Specific Supportive Text
Initial management should focus on support of the patient’s airway and breathing. This begins with opening the airway followed by delivery of rescue breaths, ideally with the use of a bag-mask or barrier device.8–10 Provision of ACLS should continue if return of spontaneous breathing does not occur.
Because there are no studies demonstrating improvement in patient outcomes from administration of naloxone during cardiac arrest, provision of CPR should be the focus of initial care.3 Naloxone can be administered along with standard ACLS care if it does not delay components of high-quality CPR.
Early activation of the emergency response system is critical for patients with suspected opioid overdose. Rescuers cannot be certain that the person’s clinical condition is due to opioid-induced respiratory depression alone. This is particularly true in first aid and BLS, where determination of the presence of a pulse is unreliable.11,12 Naloxone is ineffective in other medical conditions, including overdose involving nonopioids and cardiac arrest from any cause. Second, patients who respond to naloxone administration may develop recurrent CNS and/or respiratory depression and require longer periods of observation before safe discharge.13–16
Twelve studies examined the use of naloxone in respiratory arrest, of which 5 compared intramuscular, intravenous, and/or intranasal routes of naloxone administration (2 RCT,17,18 3 non-RCT19–21) and 9 assessed the safety of naloxone use or were observational studies of naloxone use.22–30 These studies report that naloxone is safe and effective in treatment of opioid-induced respiratory depression and that complications are rare and dose related.
Recommendation-Specific Supportive Text
Patients who respond to naloxone administration may develop recurrent CNS and/or respiratory depression. Although abbreviated observation periods may be adequate for patients with fentanyl, morphine, or heroin overdose,28,30–34 longer periods of observation may be required to safely discharge a patient with life-threatening overdose of a long-acting or sustained-release opioid.13–15 Prehospital providers who are faced with the challenge of a patient refusing transport after treatment for a life-threatening overdose are advised to follow local protocols and practices for determination of patient capacity to refuse care.
Because the duration of action of naloxone may be shorter than the respiratory depressive effect of the opioid, particularly long-acting formulations, repeat doses of naloxone, or a naloxone infusion may be required.13–15
These recommendations are supported by the 2020 AHA scientific statement on opioid-associated OHCA.3
According to the Centers for Disease Control and Prevention, opioid overdose deaths in the United States have more than doubled in the past decade, from 18 515 in 2007 to 47 600 in 2017.9 Improving recognition of opioid overdose and increasing lay rescuers’ willingness and ability to administer naloxone has the potential to improve outcomes. A scoping review was conducted to determine the impact of targeted resuscitation and naloxone training on opioid users and lay rescuers likely to encounter an opioid overdose.10 Educational interventions included training programs for family members of opioid users (including naloxone distribution), computer-based training of opioid users, peer-to-peer training (ie, opioid users teaching other opioid users), and brief counseling by emergency department staff.1–8
Educating opioid users5,7 and their friends, families,1 and close contacts5 improves willingness and ability to administer naloxone, risk awareness, overdose knowledge recognition, and attitudes toward calling EMS.3,10 We suggest that people who use opioids or those who may witness an opioid overdose receive training in responding to opioid overdose, including the administration of naloxone. The data reviewed are limited by the inability to link population-level interventions to individual patient outcomes. More research is required to determine which educational interventions provide the greatest benefit by measuring both learner and patient outcomes.
Recommendation-Specific Supportive Text
Eight studies (1 RCT and 7 observational studies)1–8 assessed the impact of opioid training using a comparator group. These studies evaluated the impact of short educational courses, with opioid users, friends, and family members as participants. Outcomes were heterogenous and included knowledge of risk, identifying overdose, knowledge and skill to respond to overdose, and willingness to aid or phone for help.1,3–8
One RCT found that 60% of witnessed overdoses involving an individual who had been trained within the prior 3 months received first aid and/or naloxone compared with zero in the comparator group.1 In an observational study, 40% of participants who witnessed an overdose in the 12 months after education administered naloxone.5 Another study found that the rate of naloxone administration was higher in those who had received opioid training compared with those who did not (32% versus 0%).4 They found no difference in the rates of calling 9-1-1 or delivering rescue breaths between the 2 groups.4 Another study found no difference in the provision of aid between trained and untrained responders.2 Interventions that included skills practice (ie, naloxone administration) were more likely to lead to improved clinical performance compared with interventions without skills practice.1,11–22
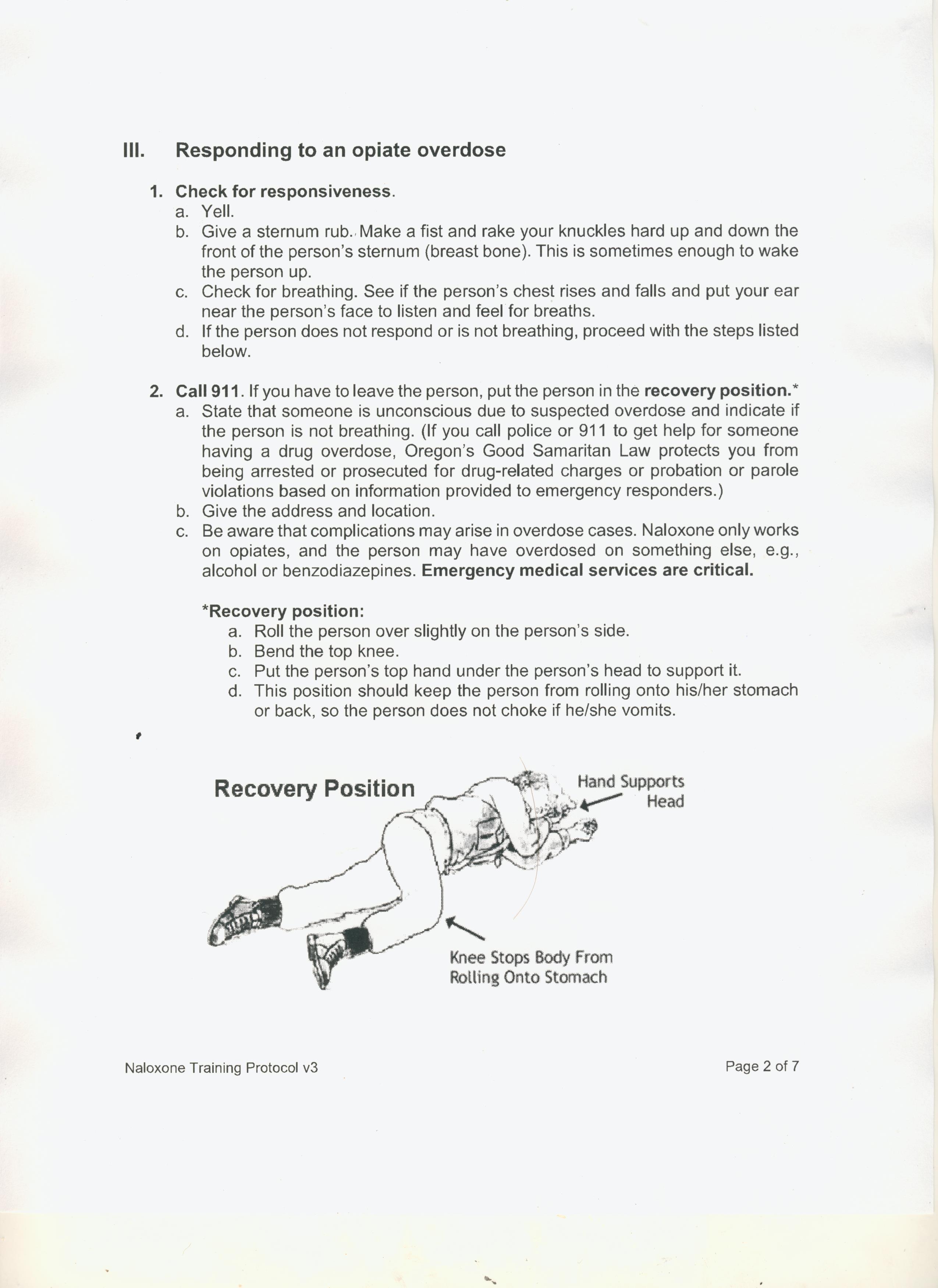
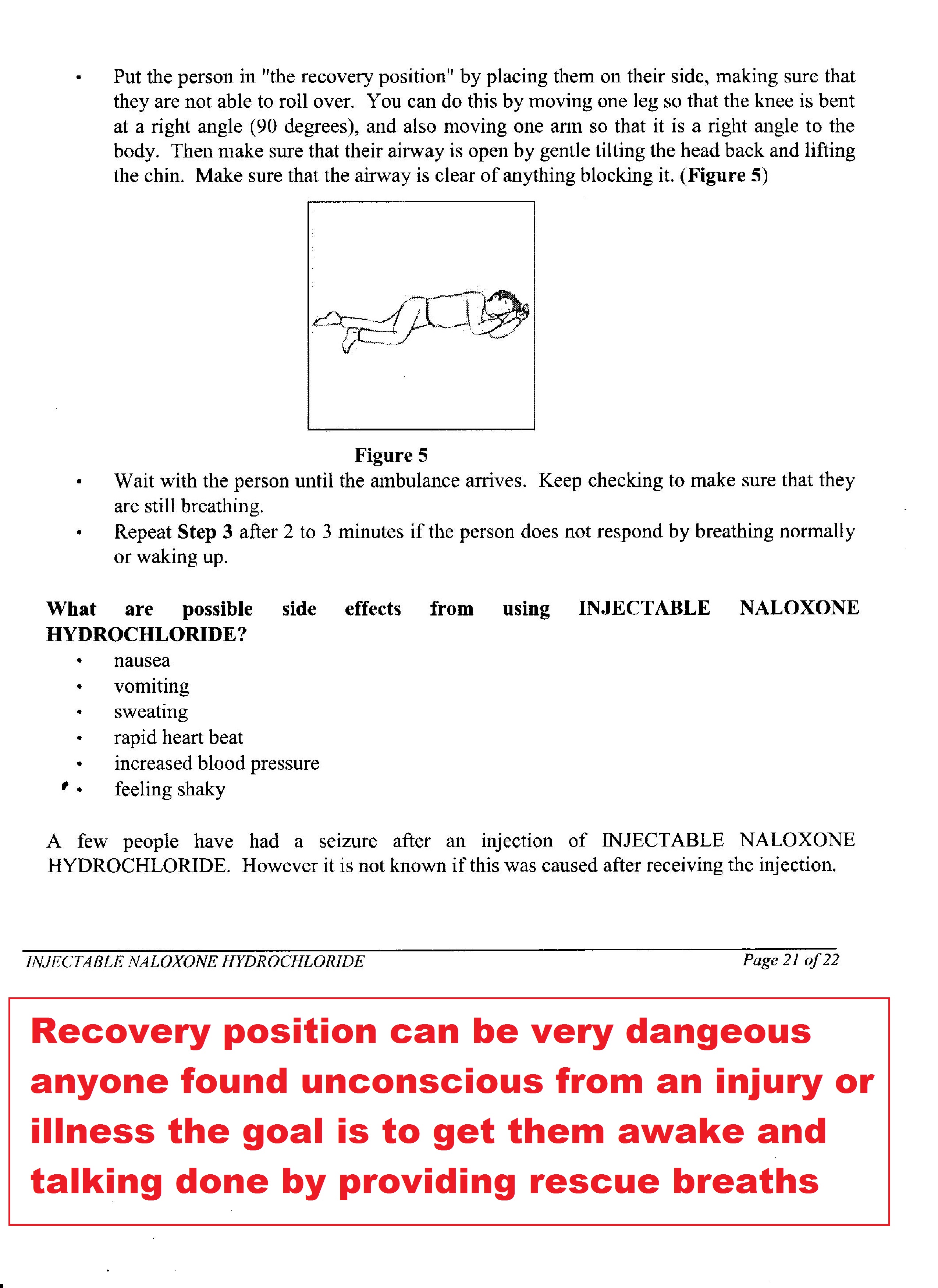
Recover position dangerous any etiology comatose, hypoxic patient goal is awaken until Glasgow Coma Scale 15 italics mine
Recovery Position for Persons With Decreased Level of Consciousness of Nontraumatic Etiology Not Requiring Rescue Breathing or Chest Compressions (FA 517: ScopRev)
Rationale for Review
The benefit of lateral positioning of adults and children with decreased level of consciousness has been widely accepted despite limited supportive scientific evidence. The most recent ILCOR evidence review on this topic in 20155,6 addressed use of the recovery position for those with decreased level of consciousness but breathing normally.
Opioid-associated deaths have increased internationally in recent years103; death is typically preceded by decreased level of consciousness and respiratory depression or compromise. Recent studies suggest that placing persons in the recovery position may hinder the detection of cardiac arrest.104–106 As a result, the First Aid Task Force sought a ScopRev on the recovery position, modifying the search strategy used in 2015 to include persons who do not meet the criteria for cardiopulmonary resuscitation but have diminished level of consciousness/responsiveness (eg, from alcohol or drug overdose, intracranial hemorrhage) coupled with breathing abnormality (ie, they are not breathing normally). The outcomes included in the search were expanded to include outcomes of hypoxic events.
The revised and updated search strategy identified more indirect evidence, such as research examining the role of patient positioning in obstructive sleep apnea and cadaver models of cervical spine instability.
Population: Adults and children with decreased level of consciousness due to medical illness who do not meet criteria for the initiation of rescue breathing or chest compressions (CPR)
Intervention: Positioning in any specific position
Comparator: Supine or other recovery position
Outcome: Any relevant clinical outcomes including but not limited to survival, need for airway management, incidence of aspiration, hypoxia, incidence of cardiac arrest (all critical); and likelihood of cervical spine injury and complications (important): venous occlusion, arterial insufficiency, left arm discomfort/pain discomfort/pain, aspiration pneumonia
Study design: RCTs and nonrandomized studies (non-RCTs, interrupted time series, controlled before-and-after studies, cohort studies) were eligible for inclusion. Case series and case reports, unpublished studies and reports (eg, conference abstracts, trial protocols, technical reports, incident reports, medical examiner and coroners’ reports) were also considered for inclusion.
Time frame: The scoping search strategy included all years and all languages as long as there was an English abstract. We reran the existing 2015 search strategy on November 4, 2019, with no date/time restrictions.
Summary of Evidence
Thirty-one studies,104,106–135 a case report,136 and 2 letters to the editor105,137 were identified from our database and gray literature search. Nine studies involved patients with a medical, medically induced, or toxicological decreased level of consciousness.105,107–112,131,136 Eight studies enrolled healthy participants,104,106,113–117,137 15 studies assessed patient positioning for ventilation during sleep,118–128,132–135 and 2 studies involved cadaveric models of cervical spine instability in recovery positions.129,130 The positions studied, airway maneuvers used, and outcomes reported in the included studies were highly variable. Seven distinct lateral recumbent recovery positions were identified, ranging from lateral to prone, and in many studies, the details of the position used (eg, degree of torso rotation, arm and head position) were not described in sufficient detail to allow for reproducibility. The comparison positions studied, when reported, were also highly variable, ranging from prone to semirecumbent and supine with manual airway maneuvers such as the head tilt–chin lift.
The gray literature search revealed a near-universal adoption of the recovery position for a decreased level of consciousness with normal breathing from unknown causes as well as known or presumed causes such as seizure, stroke, poisoning, and opioid overdose. Treatment guidelines for ski patrollers, lifeguards, prison guards, schoolteachers, and combat medics all recommended a variation of the lateral recumbent recovery position.
Most studies of the recovery position were performed in healthy volunteers (who have normal muscle tone rather than the reduced tone that may be present in an unresponsive person) and report outcomes such as dependent arm perfusion and comfort associated with positioning. For the focus area of opioid overdose, only a single study was identified, suggesting that a semirecumbent position may be preferable to lateral position.107 The First Aid Task Force agreed that additional studies are needed to confirm this finding. For other medical causes of decreased mental status, such as stroke, induced sedation, and decreased level of consciousness, the lateral recumbent position was reported to be associated with beneficial outcomes.
As noted, despite a true paucity of research to support its use, the task force acknowledged that the recovery position in its many forms has become universally recommended in first aid settings for persons with decreased level of consciousness from nontraumatic cause, provided they do not require rescue breathing or chest compressions. As a result, a change in practice will likely require substantial evidence and education.
Studies of positional interventions for sleep-disordered breathing help describe the effect of body positions on ventilation in persons with decreased level of consciousness. Most studies reviewed report lateral positioning improving outcomes of interest such as apnea, hypopnea, and oxygen desaturation. However, they may not be directly applicable to the use of the recovery position for persons with decreased level of consciousness from medical, toxicological, and nontraumatic etiology.
The task force discussion focused on the optimal position to promote adequate breathing while optimizing the detection of respiratory and/or cardiac arrest. Although the included evidence favors the use of a lateral recumbent position, the task force voiced concerns about the use of a recovery position in scenarios such as with opioid overdose when hypoxic respiratory arrest or cardiopulmonary arrest may be imminent. It is the consensus of the task force that this topic should be the subject of a SysRev in the near future.
Treatment Recommendation
This treatment recommendation (below) is unchanged from 2015.5,6
We suggest that first aid providers position individuals who are unresponsive and breathing normally into a lateral, side-lying recovery position (lateral recumbent) as opposed to leaving them supine (weak recommendation, very low-quality evidence).
Video Oct 21, 2020 AHA press release No mention rescue breaths 5 min 30 sec; 7 min 30 sec; 15 min 30 sec; 16 minutes;20 mins; 45 min 10 sec NO-NO+GO https://youtu.be/lO4rdC-fKsI
Laurie Morrison MD [co-author 2010 AHA Guidelines ‘Toxic ingestions’] quoted 15,000 out of hospital cardiac arrests per year Ontario a lot less sudden witnessed, the only time compressions only may work https://www.macleans.ca/society/health/the-heart-of-the-matter/
VI. First Aid Awareness and Training Providers of First Aid Training in Ontario, including St. John Ambulance, Canadian Red Cross, and Heart and Stroke Foundation of Canada, should:
i Ensure their standard first aid training programs and their instructors: emphasize the primary importance of airway patency and positional safety for all ill and injured patients
Liked tweet by Leah Chapman RN PhD Sister of Bradley Chapman Brad’s Mother also an RN Brad who needlessly lost his life Coroners verdict ‘Do not deny rescue breaths anyone” @NickelBelt is NDP Health Critic France Genilas who I have spoke with in person Link to coroners inquest https://twitter.com/GaryCPR/status/1205187135613153280
LinkedIn has barred me Sept 2020 for speaking a self evident truth My LinkedIn audio https://youtu.be/-pSqr0Yhjyk
Gordon Ewy MD email on the day the 2015 AHA Guidelines published His teams 20 years of research thrown down the tubes “Chest compressions only is for a sudden witnessed cardiac arrest only” Which is a very rare event
Tucson doctor a crusader for CPR change Quote “Some doctors worry that bystanders can get confused and do only chest compressions in drug-overdose and drowning cases [any asphyxia or poisoning etc italic mine] NOT TO BE GIVEN TO CHILDREN.” http://www.azcentral.com/news/articles/2010/01/19/20100119cardiacdoc0119.html
911 dispatch audio for Prince’s death April 21, 2016 [was found cardiac arrest, not much you can do in cases like his, not a simple cardiac arrest from heart disease. Clinicians worst nightmare cardiac arrest secondary to any respiratory arrest, sever brain anoxia and multiple organ system failure has occurred, oxygen deprivation] https://www.ems1.com/ems-products/communications/videos/911-dispatch-audio-for-prince-qoSt8cEvLFAgeqVV
Millions of people overdosed different substances including opioids every day around the world for surgery only thing keeping patient alive is ventilations (oxygen- rescue breaths same for layperson). Sign of overdose can mimic any of the 100s of causes breathing emergency, caused by illness or injury.
AHA Guidelines issued Oct 21, 2020 file:///C:/Users/Owner/Downloads/CIR.0000000000000890.pdf
Page 5 Resuscitation Care for Suspected Opioid Associated Emergencies Deaths from opioid overdose are increasing substantially, particularly in the United States. This topic was reviewed in 2015, but no treatment recommendation was made.12,12a An updated SysRev on this topic was considered essential to inform best-practice guidelines for bystander resuscitation for suspected opioid induced emergencies. No studies were identified that compared bystander-administered naloxone (intramuscular or intranasal) plus conventional CPR with conventional CPR only. As a response to the growing opioid epidemic, naloxone has been widely distributed by healthcare authorities to laypeople in various opioid-overdose prevention schemes. A recent SysRev identified 22 observational studies evaluating the effect of overdose education and naloxone distribution and found an association between implementation of these programs and decreased mortality rates.13 On the basis of expert opinion, the BLS Task Force suggested that CPR be started without delay on any unresponsive person who is not breathing normally and that naloxone be used by lay rescuers in suspected opioid-related respiratory or circulatory arrest.
Page 15-16 The opioid overdose crisis is recognized as a major challenge, particularly in the United States. In 2015, the ALS Task Force made a strong recommendation for the use of naloxone for individuals in cardiac arrest caused by opioid toxicity.25,26 At that time, the BLS Task Force made a weak recommendation to offer opioid overdose response education, with or without naloxone distribution, to persons at risk for opioid overdose.12,12a The EIT Taskforce undertook a ScopRev of current opioid overdose response education programs to determine whether a new SysRev is required. Of 59 studies identified, only 8 used a comparator group and only 1 was a randomized controlled trial. Inconsistent reporting of educational interventions made it difficult to compare studies, and the EIT Task Force suggests that the use of the Guideline for Reporting Evidence-Based Practice Educational Interventions and Teaching checklist would improve standardization.97 Another limitation in the evidence identified is that first aid and survival outcomes were generally self-reported by individuals refilling naloxone prescriptions and, therefore, are of questionable validity. The EIT Task Force found no evidence to change the current weak recommendation: “We suggest offering opioid overdose response education, with or without naloxone distribution, to persons at risk for opioid overdose in any setting.”12,12a
Opioid Overdose First Aid Education This topic is discussed in more detail in the EIT Hot Topics section above. The EIT Task Force undertook a ScopRev of studies that compared education about response or care of an individual by first aid providers in an opioid overdose emergency with response by those with any other or no specialized education. Among the 8 identified studies with a comparator group, the task force found no evidence to change the current treatment recommendation. Effect on treatment recommendations: The treatment recommendation is unchanged from 2015.12,12a
12. Travers AH, Perkins GD, Berg RA, Castren M, Considine J, Escalante R, Gazmuri RJ, Koster RW, Lim SH, Nation KJ, et al; on behalf of the Basic Life Support Chapter Collaborators. Part 3: adult basic life support and automated external defibrillation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015;132(suppl 1):S51–S83. doi: 10.1161/CIR.0000000000000272
12a. Perkins GD, Travers AH, Berg RA, Castren M, Considine J, Escalante R, Gazmuri RJ, Koster RW, Lim SH, Nation KJ, et al; Basic Life Support Chapter Collaborators. Part 3: adult basic life support and automated external defibrillation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation. 2015;95:e43–e69. doi: 10.1016/j.resuscitation.2015.07.041
McDonald R, Strang J. Are take-home naloxone programmes effective? Systematic review utilizing application of the Bradford Hill criteria. Addiction. 2016;111:1177–1187. doi: 10.1111/add.13326 1
Addendum
Drugs nor poisons did not magically change their chemical structure after millions of years still cause death respiratory failure. Humans still suffer myriad respiratory emergencies which can mimic overdose Correct 2010 AHA Guidelines Part 12:3 Toxic Ingestions https://heartandstroke.my.salesforce.com/sfc/p/
State sponsored psychological terrorism workplace harassment/bullying needless deaths [non ODs and ODs]; stress increasing mental/physical illness drug use/misuse. Done on purpose Be safe Be kind First do no harm @GaryCPR
Phone call July 27 Portland Public Health https://youtu.be/V1q-T4gkFQI Liz at 5 min “It’s not something I would personally teach” No sane person would teach mass murder
INCHEM is correct as per ten million references in the medical literature See part 10 Management treatment poisonings/drug OD http://www.inchem.org/pages/pims.html
Oregon Health Dept First Aid rescue breaths only, thus saving the lives any of the 100s of causes breathing emergency https://youtu.be/wsN0ijLnK2k
Jan 2017 Barbara Jaffe MD Associate Chief Medical Officer of Health and Mayor John Tory quoted “Ventilation’s (rescue breaths) most important” “This (wrong protocols) is what causes people to lose their lives quite literally” Both know they could be on the receiving end suffer any breathing emergency
In a population of 15 million over a million per year will be taken to hospital in need of oxygen (rescue breathing) large number repeat customers COPD; Asthma etc.
Same 15 million population will experience 15,000 out of hospital cardiac arrest per year. The more you teach the wrong ‘First Aid’ treatment the more likely you will be next in the morgue needlessly or drooling for the rest of your life permanent brain damage oxygen deprivation
Red arrow “If animal has a pulse continue rescue breathing” Millions trained if you have a pulse deny rescue breathing give chest compressions a beating heart killing your own children under governments etc orders
Jerome Adams MD Surgeon General quote ‘CPR’ they immediately think chest compressions It’s rescue breathing only for any breathing emergency https://youtu.be/-cjZMH_Z6Uw
Dan Bigg with Michael Parkinson Crime Prevention Council quote Dan “No brain’er rescue breathing is what it’s all about. Chest compressions are not helpful but harmful”
Jan 2017 Barbara Jaffe MD Medical Officer of Health and Mayor John Tory quoted “Ventilation’s (rescue breaths) most important” “This (wrong protocols) is what causes people to lose their lives quite literally” https://youtu.be/2Pb0HAPqWII
God is the Breath of Life
Matthew 9:24 Jesus “Go away the girl is not dead but asleep” Comatose Jesus gave rescue breaths
John 20:22 “Jesus breathed upon his disciples”
Genesis 2:7 “God breathed the breath of life into humankind”
Luke 12:4-5 Cast yourselves into hell protecting mass murder
Watching everyone’s body language give you away for years Cognitive dissonance “Strongly held belief the government MDs etc are not monsters. When confronted with the facts you will lie to yourself and others to protect that core belief which makes you physically and emotionally ill”
Mental slavery is the worst form of slavery it gives you the illusion of freedom makes you trust love and defend your oppressor while making an enemy of those trying to free you or open your eyes
Psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Increasing morbidity and mortality anyone who is alive with chest compression’s and/or oxygen deprivation”
Be safe Creator is the ‘Breath of Life’ @GaryCPR
Child knows anyone suffering any of the 100’s of causes breathing emergency rescue breaths ASAP essential The pharmaceutical companies MDs government etc USA and Canada and Europe know they are intentionally misinforming the general public. Wrong instructions increase mental and physical illness drug use misuse dysfunctional society
It was good talking with you earlier today. [I recorded phone conversation Conversation with pharmacists July 7 linked in comment box https://youtu.be/rk_lREU0vTU ]
Please find the Product Monograph for Naloxone attached with a paragraph on Respiratory on Pg. 5
Let me know if that helps your question around respiratory recovery.
Quote page 5 “”In addition to naloxone, other resuscitative measures such as maintenance of a free airway, artificial ventilation and cardiac massage could be executed by a bystander (non-health care professionals) if the bystander knows how to perform the manoeuvers”
My response Rescue breathing is essential pre Naloxone administration and afterwards. Thus saving any of the hundreds of causes breathing emergency. Note ‘cardiac massage’ is massaging the heart open chest with your hands not chest compressions.
Hi Jim:
Thanks for the quick response yes very short mention respiratory assist page 5. Also mentioned in the monograph keep giving more doses Naloxone no mention respiratory assist between administrations
Please see page 18 Omega monograph protocol no mention respiratory assist.
People have been taught rescue breathing over the phone in twenty seconds thus saving any breathing emergency
Matt Johnson and Zoe Dodd and friends 168 case reports saving non ODs & ODs teaching rescue breathing “Oxygen (rescue breaths) used more & more Naloxone less & less’ https://youtu.be/fc85iv3VQLM
Poisons nor drugs did not magically change their chemical structure after millions of years Still cause death respiratory failure
Watching everyone’s body language give you away for years Cognitive dissonance ‘Strongly held belief the government MDs etc are not monsters. When confronted with the facts you will lie to yourself and others to protect that core belief which makes you physically and emotionally ill’
Mental slavery is the worst form of slavery it gives you the illusion of freedom makes you trust love and defend your oppressor while making an enemy of those trying to free you or open your eyes
God is the Breath of Life
Matthew 9:24 Jesus “Go away the girl is not dead but asleep” Comatose Jesus gave rescue breaths
John 20:22 “Jesus breathed upon his disciples”
Genesis 2:7 “God breathed the breath of life into humankind”
Luke 12:4-5 Cast yourselves into hell protecting mass murder
Psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Increasing morbidity and mortality anyone who is alive with chest compression’s and/or oxygen deprivation”
Be safe @GaryCPR
Intersectionality is killing us all June 8, 2020 My ‘Rescue breathing’ deputation Board Health Medical references in comment box https://youtu.be/KUxzVFfg5hY
Psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Common quotes Police; Pharmacists; EMS; MDs and RNs while crying “I know they are increasing morbidity and mortality anyone who is alive with chest compressions and/or oxygen deprivation” Be safe Don’t Forget the Creators Mysteries @GaryCPR
Gary Thompson “Willfully increasing morbidity and mortality non users and users. Turning Point Naloxone: Saving Lives at 25 min https://youtu.be/scvwH9nHRzE
Graham Parsons Chief Pharmacist at Turning Point and Independent Substance Misuse Consultant
“This is disappointing. We link in with the Prenoxad and SMMGP training and understand the importance of rescue breathing for opioid overdose.
However, also need to remember that naloxone is no use on the warehouse or pharmacy shelves and having a scheme that gets it into the community is essential. Our previous schemes did not due to the length of time of the intervention and this scheme was designed after research from the University of Bath on how to get it out to clients effectively.
On a final note the current covid-19 pandemic has caused us problems with getting it out. We post now – yes post – to get it out with a call to support training. Rescue breathing would give some concern for some under the current restrictions so this may also impact on the conversation in the busy pharmacy. Bigger educational challenge is also encouraging clients to phone 999 post intervention. So don’t think this is some fly by night scheme. It is backed by research and works on the assumption that getting naloxone into the community is an essential component of reducing DRDs. If you have seen how naloxone can act in the real world – which I know you may have – you would understand. Back to my cup of tea now.
Gary Thompson “Thank you for the input. Epi-Pen/Asthma puffers etc into the community saves lives. Give public wrong instruction any medication causes harm in a thousand ways you could never dream up.
I was the 20th person trained POINT protocol Sept 2, 2011 seeking change that day onward. Not until fall 2017 were barrier masks included in the kits, wrong protocols still being taught and expanding into many health districts.
Too much fun early 2012 meeting with two public health employees “Gary there is a lot of powerful people behind this you could wind up dead” Laughed “You can’t kill me I don’t die when I die what corner what time you want me to stand there?” Put the fear of the baby Jesus into them. The creator is the ‘Breath of Life’
Layperson’s as taught eagerly denying respiratory assist giving chest compressions anyone comatose any etiology.
Teaching this malfeasance USA Canada and Europe you anyone could be next You will witness a thousand breathing emergencies ‘First Aid’ (rescue breaths ASAP) before you ever run into a cardiac arrest ‘CPR’ Signs of cardiac arrest totally different than breathing emergencies
Nova Scotia will find large percent needlessly in the morgue will be non overdoses as is happening in Ontario.
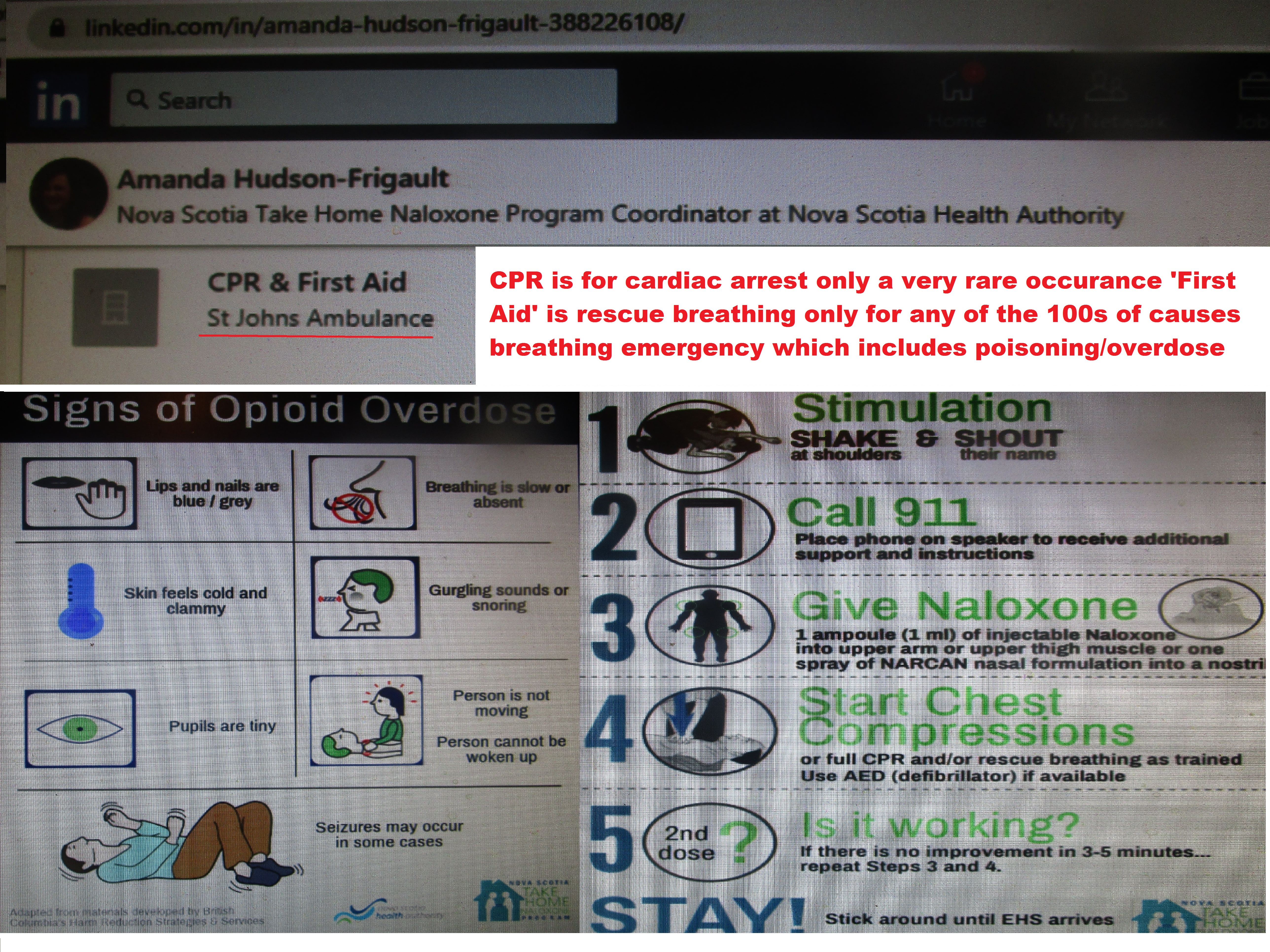
Phone call Amanda Hudson knows as any child instructions increase morbidity and mortality non overdose and overdoses
Jan 2017 Barbara Yaffe MD and Mayor John Tory quoted “Ventilations (rescue breaths) most important” “This is what causes people to lose their lives quite literally” https://youtu.be/2Pb0HAPqWII
Psychological terrorism workplace harassment/bullying needless deaths stress increasing mental/physical illness drug use/misuse. Common quotes Police; Pharmacists; EMS; MDs and RNs while crying “I know they are increasing morbidity and mortality anyone who is alive with chest compressions and/or oxygen deprivation”
Be Safe @GaryCPR











































{kind=link}